What an incredible site you have here! I was wondering if I could use one of your ECGs in my ECG course. It's the one labeled "Acute Anterior MI with AV Dissociation." This is actually a very unique and complicated ECG...
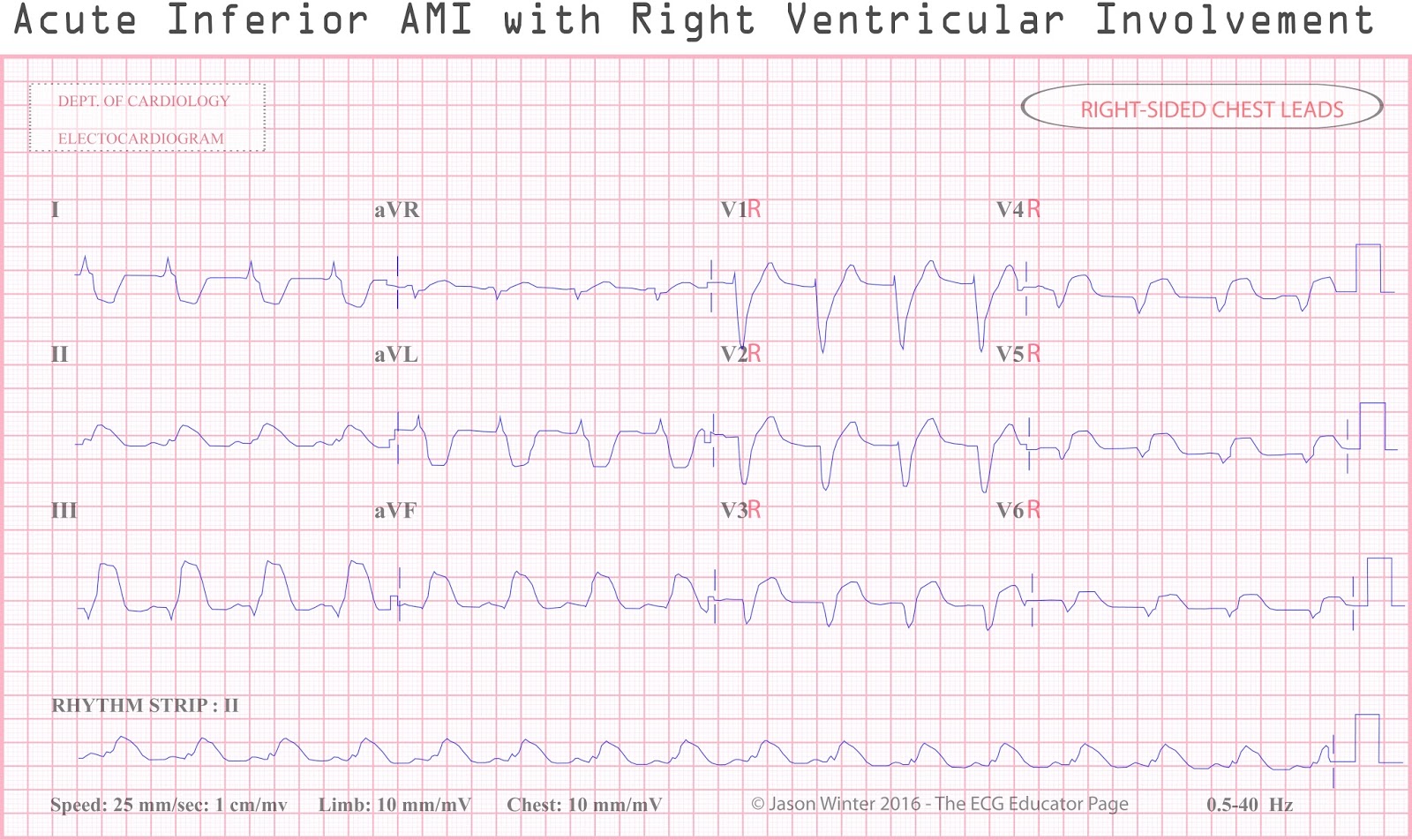
On might mistake it for a Type 3 "wraparound" LAD occlusion, but I don't think that is what has happened. A really good "rule of thumb" (though not 100%) is that only RCA occlusions with STE in the inferior leads will demonstrate any significant ST depression in aVL. For a Type 3 LAD occlusion to have STE in the inferior leads AND the ST depression of a reciprocal change in aVL would require the LAD occlusion to be distal (aVL cannot react reciprocally if it, too, is showing ischemia). However, a distal LAD occlusion is NOT going to result in STE in V1 (and often not in V2, either). So this has to be a proximal occlusion of the RCA. The "anterior MI" you have described (and - quite literally - you are correct!) is likely an acute infarction of the anterolateral wall of the RV - a right ventricular infarction. Proximal occlusions of the RCA can - at times - cause STE in ALL precordial leads. There's not much STE in Lead II because it is located on the left side of the inferior wall and that area is probably receiving circulation from the LAD and/or LCx.
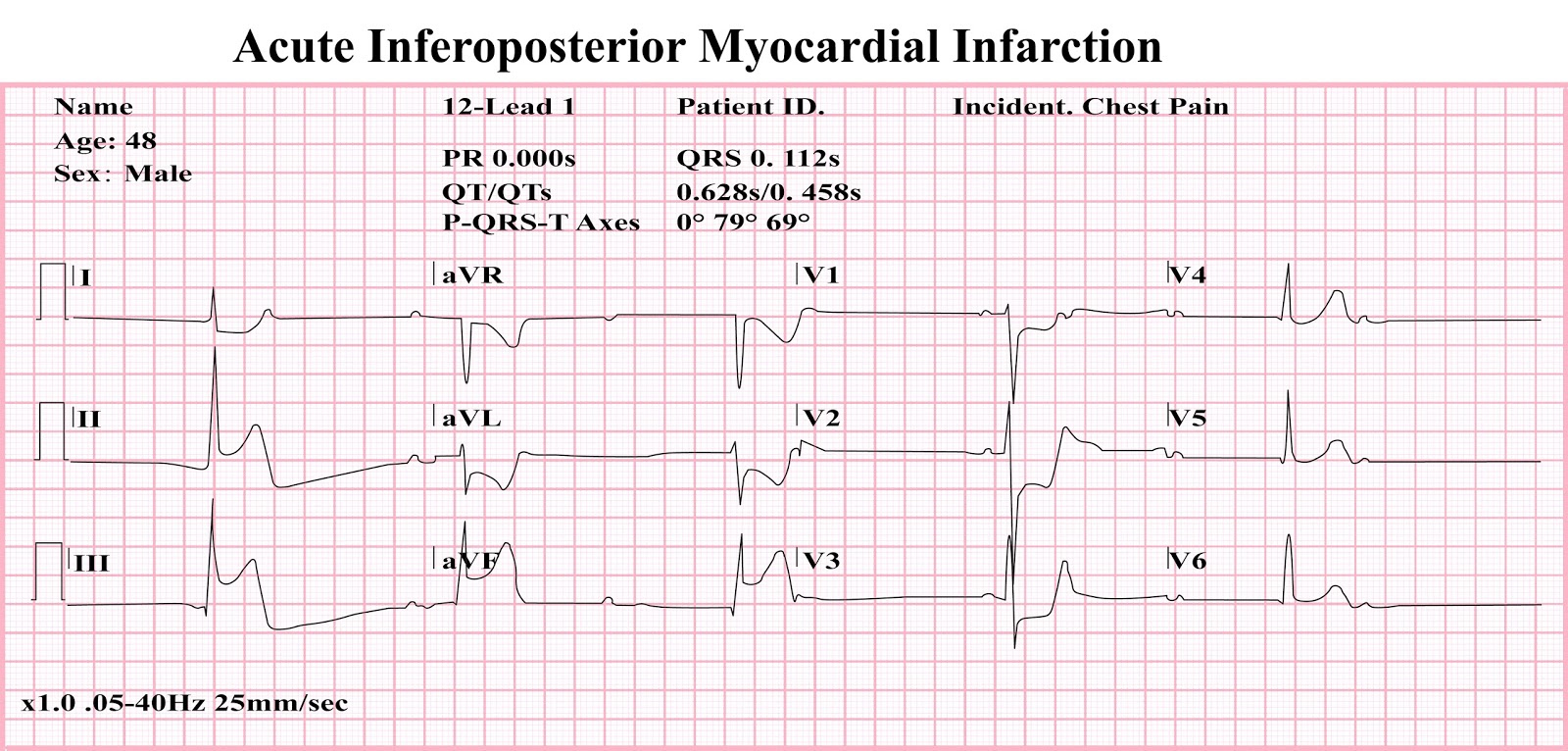
There is definitely AV dissociation present and I am very suspicious of a 3rd degree AV block since - in spite of the irregular PR intervals - the ventricular rhythm remains steady. I think the P waves in Lead V3 are in good position to have conducted. However, a longer rhythm strip would be more reassuring.
Again - congratulations on a really excellent website!








Jason!
ReplyDeleteWhat an incredible site you have here! I was wondering if I could use one of your ECGs in my ECG course. It's the one labeled "Acute Anterior MI with AV Dissociation." This is actually a very unique and complicated ECG...
On might mistake it for a Type 3 "wraparound" LAD occlusion, but I don't think that is what has happened. A really good "rule of thumb" (though not 100%) is that only RCA occlusions with STE in the inferior leads will demonstrate any significant ST depression in aVL. For a Type 3 LAD occlusion to have STE in the inferior leads AND the ST depression of a reciprocal change in aVL would require the LAD occlusion to be distal (aVL cannot react reciprocally if it, too, is showing ischemia). However, a distal LAD occlusion is NOT going to result in STE in V1 (and often not in V2, either). So this has to be a proximal occlusion of the RCA. The "anterior MI" you have described (and - quite literally - you are correct!) is likely an acute infarction of the anterolateral wall of the RV - a right ventricular infarction. Proximal occlusions of the RCA can - at times - cause STE in ALL precordial leads. There's not much STE in Lead II because it is located on the left side of the inferior wall and that area is probably receiving circulation from the LAD and/or LCx.
There is definitely AV dissociation present and I am very suspicious of a 3rd degree AV block since - in spite of the irregular PR intervals - the ventricular rhythm remains steady. I think the P waves in Lead V3 are in good position to have conducted. However, a longer rhythm strip would be more reassuring.
Again - congratulations on a really excellent website!
Jerry W. Jones, MD
Hi Jerry thanks 🙏🏻 so much, of course you can use any ECGs here, sorry only just seen this comment.
ReplyDelete